Сергей Платов
Психиатрия
Трансплантация пениса, яичек и нижней передней стенки живота

https://www.nejm.org/doi/full/10.1...
В 2018 году американские медики провели первую в мире операцию по пересадке пениса и мошонки. Реципиентом стал молодой американский солдат, который потерял половые органы и ноги после взрыва. Сейчас врачи сообщают, что реабилитация прошла успешно: пациент чувствует себя хорошо и доволен результатами процедуры. Краткий отчет и фотографии до и после операции опубликованы в журнале The New England Journal of Medicine.
До сих пор известно всего несколько случаев успешной пересадки пениса, а полтора года назад мы рассказали о пациенте, который первым в мире получил пересадку не только полового органа, но также мошонки (и участка кожи живота). Пениса и мошонки, а также ног и части тканей живота мужчина лишился в результате взрыва во время службы в армии.
После травмы уцелели лишь 1,5 сантиметра пениса с фрагментами уретры. Однако медики обнаружили, что артерии брюшной полости и малого таза у пациента также полностью сохранились, и использовали их для кровоснабжения пересаженных тканей, при этом артерии и вены пациента соединили с артерией и веной донорского пениса.
После трансплантации пациент прошел полный курс иммуносупрессии, чтобы избежать отторжения. Теперь врачи отчитались о результатах его реабилитации. В половом органе восстановилась чувствительность, хотя в головке — в меньшей степени, чем в самом теле полового члена. По словам авторов отчета, пациент может мочиться стоя (на протезах), без излишнего напряжения, и моча выходит «сильной струей». Кроме того, мужчина рассказал, что не имеет проблем с эрекцией, чувствует оргазмы и у него улучшилась самооценка.
|
|
Не у всех пациентов трансплантации заканчиваются успешно. Подробнее о том, с чем это может быть связано, читайте в нашем материале, посвященном человеку с пересаженными руками.
https://nplus1.ru/news/2019/11/08/...
Correspondence
Total Penis, Scrotum, and Lower Abdominal Wall Transplantation
November 7, 2019
N Engl J Med 2019; 381:1876-1878
DOI: 10.1056/NEJMc1907956
Metrics
To the Editor:
Male genital tissue loss can have devastating effects on sexual and reproductive function as well as on the psychosocial well-being of the injured patient. Conventional reconstructive efforts are often insufficient to restore full function of the phallus. Only four successful penile transplantations have been reported to date.1,2 We performed transplantation of the penis, scrotum, and lower abdominal wall from a young, closely age-matched donor to an injured veteran who had sustained traumatic penile loss caused by an improvised explosive device.
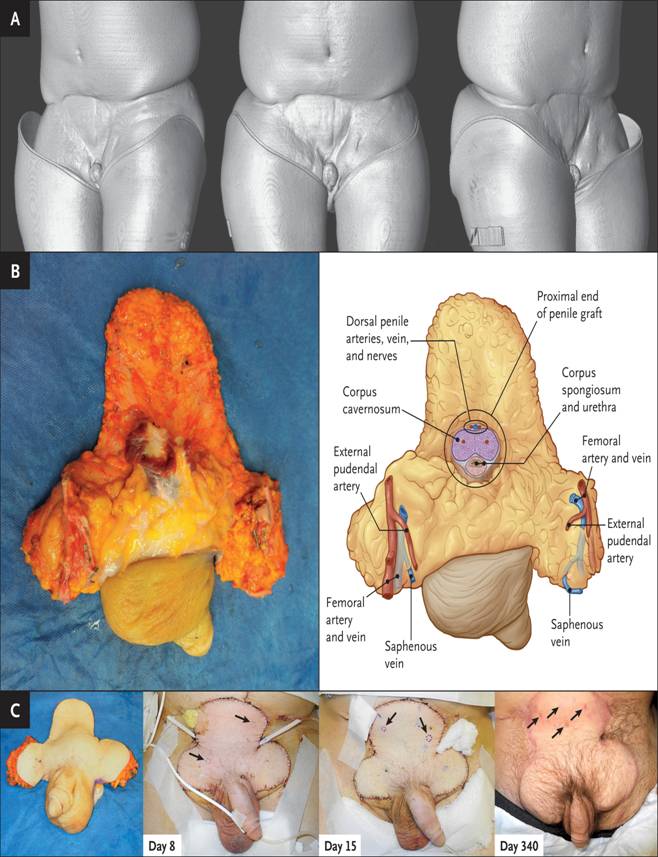
Figure 1. Transplantation of a Penis, Scrotum, and Lower Abdominal Wall.
The patient’s initial injury also included above-knee amputation of both legs, substantial tissue loss in the lower abdominal wall, and bilateral traumatic orchiectomy and loss of the scrotum. After initial healing, the patient had a 1.5-cm-long remnant of penile tissue with a urethra at the end of the amputated shaft. Scrotal tissue was absent, as were the testes (Figure 1). Preoperative imaging revealed normal bilateral inferior epigastric, iliac, and femoral arteries (Figs. S1 and S2 in the Supplementary Appendix, available with the full text of this letter at NEJM.org), but the dorsal penile and cavernosal arteries were insufficient to support transplantation. Thus, a surgical technique was developed for this patient in which the deep inferior epigastric arteries were used to revascularize the dorsal penile arteries and the graft, with the external pudendal arteries used to supplement blood supply to the tissues of the proximal shaft, groin, abdomen, and scrotum.3
The transplantation was initiated with a primary urethroplasty and corporal anastomosis. The donor dorsal arteries and veins were then anastomosed to the recipient’s deep inferior epigastric arteries and veins, and both recipient dorsal nerves were coapted to those of the graft (Figure 1). The left donor external pudendal artery was taken with a segment of femoral artery and revascularized by an end-to-side anastomosis to the recipient femoral artery with demonstrated full perfusion of the graft. The patient received alemtuzumab and glucocorticoid induction therapy, tacrolimus maintenance monotherapy, and a donor bone-marrow infusion (descriptions of the operative details and full immunologic course and treatment are provided in the Supplementary Appendix).
|
|
It has now been more than 1 year since the patient received the penile transplant. He has near-normal erections and the ability to achieve orgasm, as well as substantial improvements in pleasure scores on patient-reported outcome measures. He has normal sensation to the shaft and tip of the transplanted penis and can localize touch sensation. Neurosensory testing with the Pressure-Specified Sensory Device (AxoGen) reveals that the glans has recovered to near-normal sensibility for the one-point moving touch and has recovered to lower (better) thresholds than for the one-point static touch. Sensation in the penile shaft has recovered to higher thresholds than that in the glans. The patient urinates while standing, without straining, frequency, or urgency, with the urine discharged in a strong stream.
The patient has returned to school full time and continues to live independently using leg prostheses. He reports an improved self-image and “feeling whole” again and states that he is very satisfied with the transplant and the implications it carries for his future.
Richard J. Redett, III, M.D.
Joanna W. Etra, M.D.
Gerald Brandacher, M.D.
Arthur L. Burnett, M.D., M.B.A.
Sami H. Tuffaha, M.D.
Justin M. Sacks, M.D., M.B.A.
Jaimie T. Shores, M.D.
Trinity J. Bivalacqua, M.D.
Johns Hopkins School of Medicine, Baltimore, MD
rjr@jhmi.edu
Steven Bonawitz, M.D.
Cooper University Health Care, Camden, NJ
Carisa M. Cooney, M.P.H.
Devin Coon, M.D., M.S.E.
Aliaksei Pustavoitau, M.D.
Nicole A. Rizkalla, M.D.
Johns Hopkins School of Medicine, Baltimore, MD
Annette M. Jackson, Ph.D.
Duke University School of Medicine, Durham, NC
Vidhi Javia, B.S.
Samuel A.J. Fidder, M.D.
Janice Davis-Sproul, M.A.S.
Daniel C. Brennan, M.D.
Inbal B. Sander, M.D.
Shmuel Shoham, M.D.
Nikolai A. Sopko, M.D., Ph.D.
W.P. Andrew Lee, M.D.
Damon S. Cooney, M.D., Ph.D.
Johns Hopkins School of Medicine, Baltimore, MD
Disclosure forms provided by the authors are available with the full text of this letter at NEJM.org.